All published articles of this journal are available on ScienceDirect.

Migration of International Medical Graduates: Implications for the Brain-Drain
Abstract
Studies indicate that about 23 percent to 28 percent of the physicians working and residing in the United States, Canada, Australia, the UK and New Zealand were born and trained in the low-income countries, areas suffering from critical shortages of physicians and other health workers. In the US alone, the preponderance of the foreign physicians hails from South Africa, Philippines, India, Pakistan, and Nigeria. From Africa alone where the burden of disease, poverty, deprivation and death are greatest, around 23,000 qualified physicians emigrate annually. From the perspectives of the low-income countries, significant amounts of resources are, by necessity, committed into turning their nationals into vital intellectual capital for their own desperately needed health needs and crumbling healthcare systems. Thus, the migration of these physicians to other nations to help strengthen their already stable health care systems is not only ethically deplorable but poses moral hazards for both the physicians and the high-income countries. That is, high-income countries such as the United States, Canada, UK, Australia and New Zealand are draining the scarce recourses of the low-income countries through the loss of intellectual capital, a phenomenon that socio-economic and developmental experts have dubbed “the brain drain”.
INTRODUCTION
Illegal migration has been the bane of the US Government since the comprehensive immigration reform of 1986. This problem is compounded with the predicament of how to deal with the estimated 12 million people who are already in the United States illegally [1]. Illegal migration occupied center stage during the 2012 presidential election in the United States. Several suggestions regarding how to address this very important national crisis were offered, including deportation to countries of origin, building fences across the borders to deter unlawful entry, and Amnesty as a pathway to US citizenship.
Even so, there is a class of non-immigrants that constitutes a different social, professional-labor, and economic problem: Western-trained medical professionals, specifically physicians. Rather than asking these medical professionals to return to their countries of birth, several developed countries have created incentive-packages designed to keep them in the West, instead. In some cases, developed countries have often lured physicians already in their home countries to emigrate to the West.
This research examines the socio-economic and political correlates of physician migration. It explores factors that make destination countries conducive to the migration of physicians. According to the World Health Organization, there are about 60 million health workers across the globe [2]; however, this paper will focus exclusively on foreign physicians: those trained in both the developed and the developing countries, but end up migrating to the developed countries, principally USA, UK, Canada, Australia and New Zealand, which have been identified as the major beneficiaries of the exodus of physicians from the low-income countries [3-6].
THEORETICAL FRAMEWORK
This paper is premised on the fundamental theories of migration and the processes that facilitate the movement of educated and highly skilled individuals across national boundaries. These are the Neo-Classical Economic theory, the Remittances theory and the Historical-Structural theory. These perspectives are discussed below.
Neo-Classical Economic Theory
Neo-Classical Economic Theory explains migration in terms of the geographical differences in the supply and demand for labor across national boundaries and their wages implications [7]. Wages cause workers to move from low wage, labor-surplus regions to high-wage, labor scarce regions. The logic of the neo-classical migration model is that migrants are individual, rational actors, whose decisions to migrate are based on cost-benefit calculations [7]. That is, given the choice, including unfettered access to information, neo-classical economic framework postulates that individuals will conform to the laws of economic rationality and, therefore, would migrate to places where they would be most productive and the opportunity to earn the highest wages. In this model, the migration of labor becomes “a desperate flight from misery by impoverished people forced to migrate or a voluntary endeavor by young, ambitious people to acquire sufficient capital to invest in their own enterprise upon return” [7].
The intellectual leaders of the neo-classical economic theory are Immanuel Kant [8] and Ravenstein [9]. In his treatise titled “Eternal Peace,” Kant asserted that all “world citizens” should have a right to free movement. Kant’s philosophy of free movement of people was grounded in what he described as “humankind’s common ownership of the earth.” This right to mobility is challenged and increasingly subverted by the sovereign rights of countries to control their borders.
In his laws on migration, Ravenstein [9] concluded that migration is an inevitable part of development and that it is triggered by economic factors [10]. That is, from the viewpoint of the individual, migration is motivated by fiscal and economic considerations and the attempt to improve one’s livelihood or a country’s well-being. Therefore, people migrate in response to wage differences to maximize both their labor and its rewards [7].
Remittances Theory
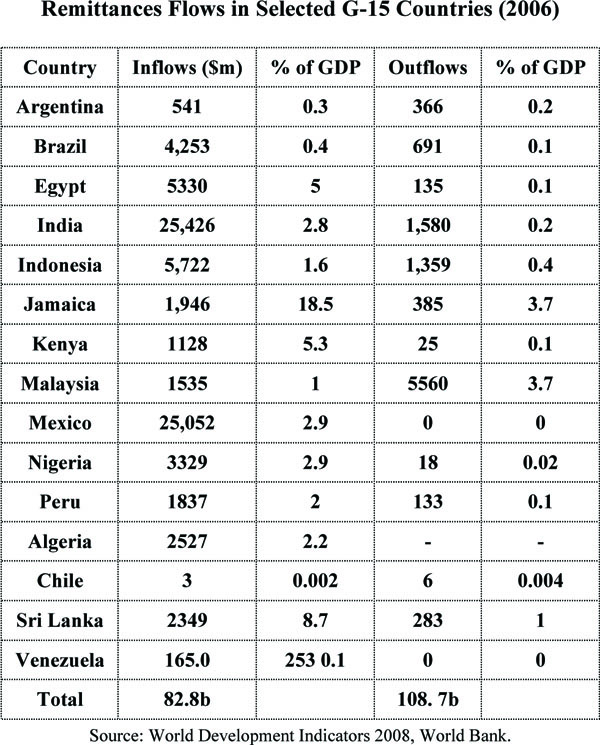
Another perspective for understanding international migration is the remittances theory. Remittances’ theory postulates that migration emanates from the desire of an individual to generate funds from the high-income countries to undertake social and economic development in the low-income countries. That is, migration facilitates the development of the donor countries [11]. Haas found that remittances to the developing countries rose from $31.1 billion in 1990 to $76.8 billion in 2000 and to $167.0 billion in 2005 [7]. According to recent studies, “migrants from the developing countries sent over $315 billion to their origin countries in 2009, three times the size of official development assistance” [12].
Research shows that G-15 member countries received $82.8 billion in remittances in 2006. India and Mexico top the list of countries that received the highest amount of remittances in 2006. With respect to remittance outflows, the G-15 was the source of 10.8 billion remittance outflows in 2006. This amounted to just under one-fourth of total outflow from all developing countries. Malaysia alone accounted for more than half the outflows of remittances from the G-15 countries [11].
Historical-Structural Theory
Another theoretical framework for understanding the migration of talents across national boundaries is the historical-structural model whose intellectual foundations are the Marxist-World Systems political and economic doctrines [13]. Historical-Structuralism posits that: (a) political and economic power are unevenly distributed between the developed and the “underdeveloped” countries; (b) that people have unequal access to resources; (c) that capitalism has a tendency to reinforce these inequalities [7]. These conditions ensure that the “underdeveloped” countries are trapped by their disadvantaged position within the global geo-political structure unable to achieve economic development and modernization.
Historical-Structuralism views migration as the natural outgrowth of the disruptions and dislocations that attenuate the process of capital accumulation. In this view, migration is one of the many manifestations of capitalist penetration caused by the increasingly unequal terms of trade between the developed and the developing countries [14]. The dysfunctions of the trade imbalance sap the creative energies of the developing economies, thus leading to underdevelopment. The lack of development, inevitably, leads to migration.
Historical-Structuralism affirms the Dependency Theory of migration [15] which postulates that global capitalism (and migration is one of its manifestations) contributed to the “development of underdevelopment”. The Dependency School views migration not just as detrimental to the economies of the “underdeveloped” countries but also as one of the very causes of “underdevelopment,” rather than a path toward development. According to this view, by uprooting their populations and undermining their economies, migration destabilizes peasant societies.
Both the Neo-classical and the Remittances migration models are based on economic and financial considerations. The desire to escape the ravages of disease and poverty and to be financially self-sufficient compels people to leave their countries in the search for the “golden fleece”. That is, the search for greater economic opportunities and higher standards of living are the predominant triggers for international migration.
Even so, there are other considerations and imperatives that pre-dispose migration, including environmental factors specific to the donor countries, violent political upheavals, general insecurities, including job insecurities, as well as religious persecution. National issues such as the economic crisis that bedeviled Spain and Europe in 2012 along with “Climate Change” as evidenced by the Sandy Hurricane that devastated eastern United States in October 2012, are phenomena which precipitated the movement of populations across State and national boundaries.
National Crises
National calamities are major drivers of international migration. Often times, these local phenomena have global ramifications. Examples include the Greek and Spanish economic implosions that resulted in a wider European economic crisis because of the interconnectedness and integration of international economies; violent political turmoil in the Arab Middle-East (Egypt, Libya and Syria) with spillover effects on Turkey and Iran; the drive toward the acquisition of nuclear capability (Iran and North Korea); and regional instability in Africa (Somalia, Sudan, Mali). These uncertainties have elevated global political temperatures compelling the citizens of these countries to seek refuge in the higher-income countries, thus increasing the need for physicians to cater to the health of the new arrivals. The physicians will come from the low-income countries, areas already suffering the burdens of critical shortages of physicians, to the high-income countries [2].
Climate Change
Climatic Change has been and will continue to be the greatest potential trigger of future international migration [16]. Migration theorists predict that as many as 200 million people may be forced to migrate by 2050 because of deadly storm surges, which would become more powerful with increased climatic warmth. A world of unpredictable and erratic climate changes will be a public health nightmare as it will be attenuated with increases in infectious diseases. Climate Change triggered Hurricanes Katrina, Isaac, Sandy, and more recently Typhoon Hyannis that rocked the Philippines. Climate Change-induced Hurricanes could displace millions of people in some low-income countries, some of whom will seek refuge in the higher-income countries, thus increasing the need for doctors in the recipient countries.
Thus, Climate Change is being increasingly perceived as public health hazard. A study by the Centers for Disease Control and Prevention (CDC) maintains that “the most obvious risk from a warming world is killer heat”. A deadly heat wave that struck Chicago in 1995 made many people aware of how disastrous sustained high temperatures can be: about 750 people died from the heat. A similar heat wave which struck Europe in 2003 killed over 70,000 people [17].
METHODOLOGY
This study is based on secondary sources: journal articles, reports and other scholarly documents, and primary data of published research, supplemented with data gathered from the departments of health and the research centers of the donor as well as recipient countries of international medical graduates. For each of the five countries, the researchers secured and analyzed the legislation and other programs they have enacted to encourage the migration of foreign physicians.
Additionally, in the United States, we conducted a survey of foreign physicians in the State of Mississippi. According to the most recent studies, there are about 777 foreign physicians in the State [18]. Out of this number, through a randomized process, 200 doctors were surveyed: every fourth physician in the state’s list of foreign doctors was sent a questionnaire to complete and to return to the researchers in enclosed, stamped, self-addressed envelopes. The survey was designed to measure the physicians motivation and attitude toward emigration. A listing of socio-economic and political factors with the potential to trigger emigration was developed and respondents were asked to identify the factors central to their decision to emigrate.
POLITICAL ECONOMY OF THE DONOR COUNTRIES
Manpower is the most important factor in any health system because the quality of the workforce determines the overall system’s effectiveness. According to the World Health Organization, there is a worldwide shortage of 4.3 million health-workers, with the shortages primarily concentrated in South Asia and Africa [2]. South Asia and Africa also bear the greatest burden of disease. Sub-Saharan Africa and South-east Asia together have 53 percent of the global disease burden but only 15 percent of the “world’s healthcare workforce” [4].
Even so, there are dynamics in the donor countries that tend to promote migration. Given good governance and internal security, better working conditions and acceptable levels of civilized conditions, many immigrants would stay home and contribute to the socio-economic and political development of their societies. However, these rudimentary necessities of personal survival are lacking in the principal donor countries: Pakistan, India, Nigeria, South Africa and Haiti, thus pre-disposing their physicians to the attraction of international migration. A review of each country is presented below:
Pakistan: Pakistan is economically poor and with a checkered history of instability. Apart from the constant threat of war with India over the Kashmir territory and the mistrust of Afghanistan over alleged Pakistani sponsorship of the Al-Qaida terrorism, Pakistan has suffered major political set-backs: the secession of Bangladesh from Pakistan with the tacit support of India and the on- and off- war with India over the ownership of Western Kashmir.
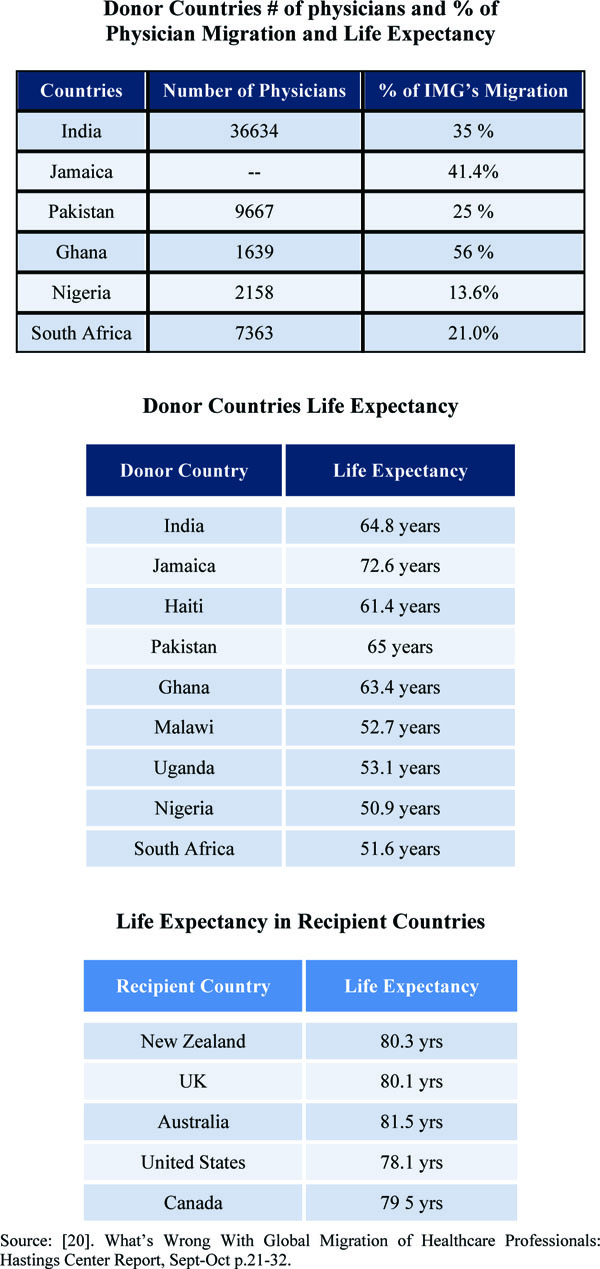
These unstable dynamics keep Pakistani citizens constantly on edge and feeling insecure. Thus, Pakistani physicians have no qualms considering emigration to the West in search of economic opportunities and better working conditions. Pakistan is ranked 122nd on the World Health Organization’s ranking of the world’s health systems. In 2010, Pakistan had 0.73 physicians per 1,000 population [4]. Malik et al. also noted that in 2005, Pakistan had approximately 74,000 physicians and about 1,700 or 2.3 percent of its physician population, emigrate every year. Yet, Pakistan’s life expectancy is only 65 years.
India: With a population of more than one billion people, India is the second most populous nation in the world. India is in a never-ending war with Pakistan over the disputed Kashmir territory. Internally, India is under constant siege by Sikh separatism and nationalistic aspirations. With numerous institutions of higher learning, India produces many physicians each year. But these doctors end-up migrating to the West once they have completed their medical education. Many hospitals in many high-income countries are populated by Indian physicians. Almost 60,000 Indian physicians practice in the US, the UK, Canada and Australia, a workforce equal to 10 percent of the physicians in India and the largest émigré physician workforce in the world [19]. Meanwhile, life expectancy in India is only 65 years.
Nigeria: Nigeria is the most populous country in Africa. With a population of 160 million people, an economy in shambles, the country is mired in poverty, disease, and a physician migration rate that has virtually crippled the country’s healthcare system. Migration of physicians has been aided by political uncertainty, the lack of investment and job opportunities. Complicating the situation is the spate of political assassination and other forms of violence, including the kidnapping of international investors and holding them for ransom. The situation in Nigeria has been so dire that the US intelligence agencies have predicted the looming demise of Nigeria by the year 2020. These predictions encourage Nigerians of all walks of life, especially physicians, to consider emigration in the face of a life expectancy of 50.9 years in 2007.
South Africa: South Africa carries the baggage of “apartheid,” which had been dubbed the worst form of enslavement and discrimination in human history. Rich in gold and intellectual capital, South Africa’s colorful past remains a burden causing most of her skilled nationals, especially Blacks, to emigrate. Indeed, many of South Africa’s Black physicians live and work outside of the country. With a deplorable life expectancy of 52 years and a wretched healthcare system, South African physicians have a tendency to migrate. Recently (2012), the country experienced a violent labor unrest that resulted in the death of thirty-four gold miners. Taking together, these make South Africa an unsafe and un-nurturing environment for her healthcare professionals, especially Black physicians.
Haiti: Haiti has the distinction of being the poorest country in the Western hemisphere. Political instability and frequent riots have rendered the country virtually ungovernable. Since 2004, Haiti has had six presidents. In 2011, a massive earthquake resulted in the deaths of thousands of Haitians and devastated its economic and social infrastructure. The physicians who survived the earthquake are either stoically helping to rebuild their country’s shattered medical infrastructure or migrated to other countries.
Thus, all the donor countries have systemic issues, ranging from war and political conflicts, the lack of infrastructure, including medical infrastructure, an irresponsible political class that has ignored the grave situation facing their countries. All of these have led to the flight of their skilled medical professionals to other countries.
Recipient Countries
Mullan [19] found that international medical graduates constituted between 23 percent and 28 percent of the physicians in the US, UK, Canada, Australia and New Zealand with the low-income countries supplying between 40 and 75 percent of them. India, the Philippines, and Pakistan are the leading sources of international medical graduates. The UK, Canada, and Australia draw a substantial number of physicians from South Africa, and the US draws most of its international medical graduates (IMGs) from the Philippines and Nigeria. Nine of the countries with the highest emigration factors are in Sub-Saharan Africa or the Caribbean. Below is a review of the internal dynamics, including polices created by the high-income countries to lure international medical graduates to their shores.
United States of America: Many rural areas in the United States are facing shortages of physicians that could imperil their healthcare delivery systems. Unable to entice American-born physicians to locate in their communities, rural areas have turned to foreign-born physicians to cater to the health needs of rural populations. Even the US Government has also turned to foreign physicians to plug the gap in physician shortages by crafting an array of incentive policies to aid the recruitment and retention of foreign physicians who are willing to live and practice medicine in clearly identified rural communities in the United States. The package of incentives include: a one year Practical Experience or Internship following the completion of the foreign student’s medical education, Loan Forgiveness Programs and Visa Programs that provide a faster track to American citizenship. These programs have also been extended to foreign-born and foreign-trained physicians to encourage their emigration to the United States.
The J-Visa program was established in 1994 to address the shortage of physicians in rural, medically under-served communities. Known as Conrad 30 or State 30, this visa waiver program was designed to encourage physicians to establish practices in the rural areas. It offers foreign-born doctors on student (F-1) visas a pathway to permanent residency in the United States, if they agreed to work in a rural, under-served area for three years. This opportunity has enabled hospitals and state agencies to recruit and to retain the best foreign-born doctors and to stabilize their healthcare workforce.
Under Conrad 30, each state is allowed 30 slots of new graduates or immigrant doctors per year. Conrad 30 waivers’ target primary care physicians who have completed a US residency training program in Family Medicine, General Obstetrics, General Pediatrics, General Medicine or General Psychiatry [21]. Prior to the enactment of this legislation, US-trained foreign physicians were required to return to their countries of origin for two years before they were eligible for emigration to the United States [22].
The Federal Government operates, through the National Health Service Corps (NHSC), a students’ loans forgiveness program for health professionals, especially physicians, who agree to practice for at least three years in a rural area. In addition, the NHSC also awards matching funds to states to operate their own loans repayment or abatement programs. For example, in Nebraska, physicians, dentist, and clinical psychologist can receive up to $40,000 per year for 3 years if they locate their practice in the Nebraska Rural Health Advisory Commission designated shortage areas [23]. This liberal provision explains why “25 percent of practicing physicians in the US and 28 percent of US medical residents come from abroad. Of these, 25 percent were trained in India and Pakistan, countries with health worker crises so acute that the World Health Organization included them on its list of countries with a “Human Resources for Health Crisis” [24]. In 2011 each country had a mere 1.13 doctors per 1,000 inhabitants, while the US enjoys 13.22 per 1,000 populations, one of the highest in the world [24]. Many other developing countries have already lost more than half of their physicians to the US. For example, there are more Ethiopian physicians practicing in Chicago than in all of Ethiopia, a country of 80 million people [24].
New Zealand: New Zealand relies on IMGs in staffing its medical workforce [25]. The number of registered, active doctors in New Zealand in 2010 was 13,883, which represented 41.1 percent of the health workforce in the country and one of the highest in the Organization of Economic Co-operation and Development (OECD) countries [25]. Although New Zealand produced more medical graduates per 10,000 population in 2009 compared to Canada, the US, Australia and the UK, these were insufficient to address the medical needs of the country. While in 2007 the OECD countries averaged 180 specialist doctors per 100,000 population, in New Zealand that average was 317 doctors per 100,000 population [25]. Even so, Parliament still enacted a series of legislation designed to attract and retain physicians in the under-served areas of the country.
In 2009, a program which provides incentive payments for up to five years to assist with student loans of medical, midwifery and nursing graduates who work in hard-to-staff locations was enacted. Health Workforce New Zealand (HWNZ), in conjunction with the Auckland District Health Board, also offers a 12 Week program to assist IMGs prepare for the Medical Council of New Zealand Registration Examination [25]. These are significant steps designed to assuage New Zealand’s critical shortage of physicians.
Britain: Doctors from outside the European Union are required to be registered to work in Britain. They must, in addition, secure a license from the General Medical Council (GMC) of the United Kingdom in order to practice medicine. In addition, immigrant doctors must secure one of three types of registrations from the GMC: Full, Limited, and Specialist. Full Registration allows certified medical doctors, who are citizens of the European Economic Association (EEA) to undertake paid unsupervised employment in the UK [26]. Limited Registrations’ is awarded to physicians whose medical credentials have been vetted and recognized by the GMC. The applicant must also take and pass the Test of English offered by the International English Language Assessment Service and the Professional and Linguistic Training Board (PLAB Test). Specialist Registration status is reserved for specialist physicians, who serve as consultants. When appropriate registration or licensure has been attained, doctors will then apply for UK migration visa-either the Work Permit or the Tier-1 General Skilled Visa.
Canada: Canada has an acute shortage of physicians, which has been exacerbated by physicians’ retirements and the “brain drain” that has been pulling young Canadian doctors into the United States [5]. As the demand for physicians soared, Canada has relied on IMGs to supplement her needs. In 2002, IMGs represented 22.7 percent of physicians in Canada, which constituted 22.5 percent of family physicians and 22.8 percent of specialists physicians in the country [5].
Physicians are unevenly distributed in the country, with rural communities bearing the brunt of the problem. In 1996, only 9.8 percent of physicians were practicing in rural Canada, where 22.2 percent of Canada’s population lived” [27]. Rural Canada is characterized by “a smaller range of healthcare providers, rural hospital closures, and centralized heath services, all of which have negatively impacted rural residents who, studies indicate are ageing more rapidly than their urban counterparts” [27].
Canada has developed an array of strategies and incentives programs to entice physicians to the rural and remote areas, which explains why each year roughly 400 foreign physicians migrate to Canada [27]. Policies that have been designed to encourage migration can be grouped into four categories: regulatory/administrative, financial, educational, and “laissez-faire” or market solutions” [27].
Administratively, the Canadian Government instituted a policy of a mandatory two-year rotating internships in the rural areas. Financially, the Government guaranteed minimum income contracts, rural/remote isolation allowances, loan forgiveness programs, assistance with practice expenses, and differential fees for serving in hard to-supply areas [5]. Other incentives include signing bonus for doctors who agree to practice in rural, shortage areas (British Columbia) and Free Tuition Program which provides up to $40,000 to final year medical students, residents and newly graduated physicians in exchange for a full-time service commitment in an underserved area in the province (Ontario). Finally, is the “laissez-faire” approach, which postulates that as urban centers become over-supplied or saturated with physicians, thus depressing service charges and physicians incomes, new physicians will slowly begin to locate in the rural and areas. That is, overtime, the market will correct the physician imbalance.
Australia: Australia has elaborate requirements for health workforce migration. Doctors who wish to practice in Australia must first register with the Medical Board in the State or Territory, where they intend to practice [28]. Overseas-trained doctors and foreign doctors, who are graduates of Australian medical colleges, must secure the approval of the state or territory in which they intend to practice medicine. After visa is granted, doctors must apply to Medicare Australia for a Medicare Provider number [29]. Doctors who secure Full Medical Registration would be eligible to migrate to Australia. Graduates of Australian medical schools or New Zealand Medical Council accredited medical schools and who complete their internships in Australia, are eligible to apply for one of the following: Occupational Trainee Visa (4 42) or Temporary Business (Long Stay) Visa (4 57) in order to work in Australia [29].
Results of a Survey of IMGs in One State: In 2011, the authors conducted a survey to assess the impact of migrant physicians in the health of rural populations of Mississippi. The choice of Mississippi as the unit of analysis was deliberate: the state is mostly rural and with the highest prevalence of cardiovascular diseases in the nation. The questionnaire addressed the following issues: (a) Physicians’ countries of origin, (b) why they emigrated to the United States and the State of Mississippi, (c) medical specializations, (d) location of practices (rural or urban), (e) factors that informed their decision to locate in the rural areas of the State, and (f) impact of the migration on their professional growth and development.
The survey response was poor, given that 200 questionnaires were mailed to 200 randomly selected foreign physicians and only 47 responses were returned, despite repeated solicitations. This represents approximately 23 percent return. The paucity of response may be due to laxity on the part of the physicians, the lack of staff time to complete the questionnaire or irregular and unreliable mail deliveries, given the rural nature of the State.
Discussion of Survey Results: An analysis of the 47 respondents, found that the majority of the foreign physicians in Mississippi come from Asia, which includes India and Pakistan: 18 out of 47 or 38.0%; Europe, 10 or 21%, the Middle-East, 9 or 17.0%, the Caribbean Island, 5 or 11.0 %, and Africa, 3 or 7.0% and 2 or 4.0% of the physicians come from the US Territories. This result is consistent with other surveys: most of the foreign physicians in the US come from Asia, principally India and Pakistan. Asked to identify their areas of specialization, 50 percent of them identified primary care, a specialty that is in high demand across the United States. With respect to the location of their practices, nearly 100 percent of the respondents identified a rural medically under-served county in the State of Mississippi, (consistent with their visa conditions and loan forgiveness agreements).
Survey participants were provided a list of migration pre-disposing factors and asked to rank the power of each factor in their decision to migrate. Working conditions was ranked first. Ranked second was quality of life, including the inadequacies of medical infrastructure. High crime activities (kidnappings, armed robberies) in their home countries ranked third. Ranked fourth was war and political conflicts in their home countries; the desire to live in an economically stable country; ranked fifth. Enhanced medical technology ranked a distant sixth.
Survey respondents were also asked to assess the impact of migration on their countries as well as on the host country, the United States. They noted that for their home countries, the impact is mixed and for the recipient or host country, the impact is very positive: without the IMGs, rural health will suffer. The limited participation of the foreign physicians in the survey does not diminish the validity of the findings, because the authors conducted informal telephone interviews of foreign physicians who are working in the metropolitan, urban areas of the State. Their responses were consistent with those of their rural counterparts. That is, the findings of the study can be generalized.
Implications for the Brain Drain: Brain Drain is the movement of educated and talented peoples from one country to another. The term brain drain was coined by the spokesperson of the Royal Society of London to describe the outflow of human capital, scientists and technologists from Britain to the US and Canada in the1950s, in search of employment, trade, and education, and social benefits [30]. This phenomenon is also known as the relocation of intellectual human capital from developing to developed countries [30]. Tahir et al.; also found that about 6 percent of the world’s physicians (140,000) resided outside their countries of birth and that 90 percent of all migrant physicians moved to just five countries: Australia, Canada, Germany, UK and USA.
Migration has worked to the detriment of the low-income economies. Rather than be a path toward development, it has been cited by the historical-structural theorists as one of the causes of under-development [7]. According to this perspective, by uprooting their populations and undermining their economies, migration destabilizes whole peasant societies. Physician migration has led to a devastating loss of desperately needed intellectual capital, especially medical talents, from the low-income countries, resulting in increased disease and early deaths in the low-income “donor” countries. The “brain drain” has also led to the lack of medical infrastructure and the perennial insufficiency of physicians that are desperately needed by the low-income countries to meet their growing healthcare needs. The migration-induced shortage of physicians has become a significant impediment to the provision of healthcare in the low-income countries. The brain drain reflects the loss of public resources invested in the education of the physicians and to the reduction in production capacity. It has led to the establishment of new medical schools to produce physicians to mitigate the adverse impact of the migration, thus creating additional fiscal burdens.
The brain drain or the migration of intellectual capital to the developed countries has retarded the development of democratic political institutions and values in the low-income countries. That is, the emigration of a critical mass of educated and capable individuals has led to loss of governance capacity in the low income countries, all of which have weak political institutions and varying degrees of instability. According to Delgado, emigration negatively impacts donor-countries in another way: it can be a mechanism for the release of political pressure on the regime diminishing the incentives for political reform, the elimination of corruption and governmental effectiveness [31].
Physician migration and the continuing loss of intellectual capital would be exacerbated by the US Patient Protection and Affordability Care Act of 2010. The Affordability Care Act would have severe cost consequences for the low-income countries given research that indicates that the reform will pull into the healthcare system an estimated 32 million uninsured Americans. Its full implementation will create the demand for qualified doctors and nurses to the United States, lured by higher salaries, including better working conditions [31]. That is, the Act will trigger an exodus of doctors from their home countries to the United States to meet the growing demand for medical doctors [25]. According to Tulenko, as many as 150,000 additional doctors will be needed by the US in the next 15 years to fully implement the Affordability Care Act [25]. These doctors can only come from the overseas, especially the low-income, developing countries because the U.S. domestic educational system, cannot, in the short-term, produce enough doctors to cater to the needs of the new entrants into the healthcare system. Thus, upon implementation in 2014, the Affordability Care Act would induce a massive brain drain of medical professionals, a frightening prospect for the cash strapped nations that cannot compete with the higher salaries, sophisticated medical technologies and other accoutrements that accompany US medical and healthcare delivery services and practices.
When significant numbers of doctors migrate, their countries lose the return on their investment on the physicians. These countries also face weakened health systems. With fragile health systems, the continuing loss of intellectual capital can bring the entire system close to collapse, with devastating consequences.
Several studies have calculated the financial costs and benefits of the brain-drain. According to Kelland, “Sub-Saharan African countries that invested in training doctors have ended up losing $2 billion as the physicians leave home to find work in more prosperous developed nations” [32]. A study by Canadian scientists found that South Africa and Zimbabwe suffer the worst economic losses due to doctors emigrating, while Australia, Canada, Britain and the United States benefit the most from recruiting doctors trained abroad. The study found that the benefits of foreign migration from Sub-Saharan African to Britain was around $2.7 billion, and to the United States around $846 million, Australia was estimated to have benefited to the tune of $621 million and Canada, $384 million [33]. Many wealthy destination-countries, which also train fewer doctors than they require, depend on immigrant doctors to make up the shortfall.
Developing countries are effectively paying to train physicians that then support the health services of developed countries. The “brain drain” of trained health workers from poorer countries to richer ones exacerbates the problem of already weak health delivery systems in low-income countries that are battling epidemics of infectious diseases such as HIV/AIDS and tuberculosis (TB) and malaria. The inadequacy of physician workforce in many of the donor countries has become a major impediment to disease reduction initiatives sponsored by international organizations, such as the Global Fund, the WHO, the World Bank and the US Government. That is, the brain drain has reduced the capacity of the “donor” countries to respond to crippling and debilitating infectious diseases [30].
CONCLUSION
Physician migration has been the bane of the rich Anglophone health systems as the reluctance of native born physicians to service rural populations has led to a reliance on foreign physicians to service these areas. The financial lure of the West, coupled with better working conditions as well as liberal immigration policies have led to an in-flow of physicians from the low income countries to the rich countries of Europe, America, Canada and Australia, including New Zealand. The result is a debilitating brain drain. The migration of physicians from the poor to the rich countries has contributed immensely to the growing health-workforce crisis in the developing world [4].
Even so, some studies have found that physician migration has spurned social and economic development in the low- income “donor” countries and to the development of advanced health knowledge that has enabled reductions in the rates of infant mortality and overall death burden for the general population.
To stem the brain drain, low income countries must improve domestic training of physicians and develop policies that facilitate the return of migrants. This will include better working conditions across the board, especially in rural and remote areas. Similarly, high-income countries must also work to eliminate their dependency on migrant physicians by educating and training more of their own nationals in medicine and making better use of the existing pool of physicians. This can be achieved by making service in rural communities a condition for graduation. Additionally, there must be responsible recruitment policies by destination countries coupled with fair treatment of migrant health workforce.
ABOUT THE AUTHOR
Dr. ‘Emeka O.C. Nwagwu is a professor of health policy and management in the School of Health Sciences, College of Public Service, at Jackson State University. His research interests include health policy analysis, healthcare finance, public health advocacy and international health.
CONFLICT OF INTEREST
The author confirms that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Thanks to my colleagues Dr. David Brown, Dr. Mohammed Shabazi and Dr. Delicia Brown-McGee, who painstakingly sorted-out the Vancouver style of footnoting and references format. I owe them a debt of gratitude. I am equally indebted to Ms. Edith Offiah, my graduate assistant from 2011-13, who conducted the preliminary research that gave reality to this article.

