All published articles of this journal are available on ScienceDirect.

Validity and Reliability of the Greek Version of the Literacy Assessment for Diabetes Scale
Authors Info & Affiliations
Abstract
Background
The Literacy Assessment Scale (LAD) for diabetes is a tool used to assess Health Literacy (HL) in patients with Diabetes Mellitus (DM). The purpose of this study was the translation, cultural adaptation, and evaluation of the validity and reliability of the LAD scale in Greek.
Methods
The research was carried out in health centers in the region of Attica, from October 2019 to February 2020. The reverse translation method of the original version of the LAD scale was adopted, with translation from English to Greek and vice versa, by two experts working independently. The scale includes 60 words in three columns of graded difficulty and increasing complexity, assessing the pronunciation of each word. Validity and reliability testing were performed on a sample of 50 adults with DM. In order to check the content validity, a pilot study was carried out with ten patients. The results added two additional subscales to assess knowledge and comprehension of each word. The level of statistical significance was set at p<0.05.
Results
The majority of participants were married men (58%), with a mean age of 68 years. Cronbach’s alpha coefficients were 0.87, 0.86, and 0.92 for the subscales “pronunciation,” “knowledge,” and “comprehension,” respectively. The mean score for the “pronunciation” subscale was 56.76 (± 3.75), for “knowledge” it was 54.28 (± 4.34), and for the “comprehension” subscale, it was 48.92 (± 7.05). In the adaptive percentage performance of the verbal assessment, both “knowledge” and “pronunciation” subscales were rated above 90%. Statistically significant differences were found in the “pronunciation” (p < 0.001) and “comprehension” (p < 0.001) subscales among employed persons under 67 years of age compared to those aged 67 and over, unemployed, or retired. Additionally, statistically significant differences were observed in the “comprehension” subscale (p < 0.001) between tertiary education graduates and those with primary or secondary education.
Conclusion
The Greek LAD scale is a reliable and valid tool to assess HL of patients with DM. It is a quick and easy-to-use tool for nurses providing healthcare to people with DM in the community. Nevertheless, this scale needs further psychometric validation in other populations, settings, and countries.
1. INTRODUCTION
Health Literacy (HL) encompasses the cognitive and social skills that determine an individual’s motivation and ability to access, understand and use information in ways that promote and maintain good health. At the same time, HL is a means of developing both individuals and society as a whole, as it improves citizens' access to health-related information and their ability to use it [1].
The World Health Organization (WHO) has defined HL since 1998. HL is a concept that represents the cognitive and social skills determining an individual’s ability and motivation to access, understand, and use health-related information to promote and maintain good health. Achieving this goal requires knowledge, personal skills, and confidence, which are crucial factors in improving both individual and community health by influencing behaviors and living conditions [2, 3].
According to modern perceptions of health, people actively participate in controlling their health by making the right decisions. Good decisions require skills in understanding and utilizing health promotion information. These skills have been characterized as HL [4]. Its important contribution as a determinant of health is widely recognized, which is why HL has been increasingly prioritized in public health policy formulation by national healthcare systems over the past decades [5]. Despite its importance and critical role, studies focusing on HL remain limited. Although several assessment tools exist, there is a general consensus that HL lacks a single, comprehensive tool for its measurement [6]. In the management of chronic conditions, such as diabetes mellitus (DM), practical skills are often more directly linked to individuals' self-care needs [7], while low HL can act as a significant barrier to effective self-management [8].
According to the data by the WHO, diabetes mellitus (DM) is among the 10 leading causes of death worldwide, responsible for 1.5 million deaths [2, 9]. The assessment scales of HL in DM care are constantly expanding and improving. Core scales have been constructed and are used in the context of HL assessment and the development of educational interventions for people with DM. These scales assess the ability to read, pronounce, and understand words related to DM, as well as the ability to perform basic numerical calculations. Several scales incorporate one or more of these skills related to DM self-management and are available in English and other languages [10]. For community nurses, HL assessment scales are useful tools in effective communication with people with DM and their self-care. Reading fluency does not necessarily presuppose the ability to understand the meaning of words and concepts. However, the cognitive processes required to understand spoken and written instructions are directly related to an individual's verbal and numerical ability [3].
The HL scale, known as the Diabetes Literacy Assessment Scale (LAD), is designed to measure the verbal ability of individuals with DM in reading words of graded difficulty. These words are related to terms and concepts commonly encountered in daily life and specifically relevant to DM care [11]. The LAD is a reliable and valid tool for assessing HL in adults with DM. In addition to its original English version, it has recently been translated and culturally adapted into Arabic [12]. However, the LAD scale has not yet been translated, culturally adapted, or validated in the Greek language. Therefore, the purpose of this study was to translate, culturally adapt, and evaluate the validity and reliability of the LAD in a Greek population with DM.
2. MATERIALS & METHODS
2.1. Design & Setting
A cross-sectional and quantitative study was conducted from October 2019 to February 2020. The study took place in the community health centers of the 2nd Health Region of Piraeus and the Aegean.
2.2. Sample
Through convenience sampling, 50 adults with DM were recruited. They attended the regular outpatient clinics of the community health centers.
This sample size was selected based on feasibility considerations and in alignment with similar validation studies of translated HL tools, where sample sizes of 30 to 60 participants were commonly used for initial psychometric evaluation. While a formal statistical power calculation was not conducted, the sample was deemed adequate for initial validation, internal consistency testing (Cronbach’s alpha), and exploratory group comparisons.
The inclusion criteria for the study were: individuals diagnosed with diabetes mellitus, aged over 18 years, with a diagnosis duration of at least one year, and the ability to speak, read, and understand the Greek language. The exclusion criteria included individuals with mental or psychiatric disorders, those who do not speak or understand Greek, individuals under the age of 18, and those with sensory impairments (hearing or vision).
2.3. The LAD Scale
At first, permission was obtained from the original developers to translate and culturally adapt the LAD. To ensure the quality and efficiency of the tool for measuring oral reading and comprehension in the Greek population, the process was carried out in two phases. The first phase included the translation of the tool, using forward-backward translation, and the second phase included the application of the tool to a sample of 50 people with DM, older than 18 years.
The LAD translation process followed the standard backward translation method, beginning with a translation from Greek to English. Researchers involved in the reverse translation worked independently to ensure the conceptual consistency of the scale's words and terms. Subsequently, two experts in primary health care assessed the conceptual equivalence of the translated terms. Finally, the researchers conducted a comprehensive review to finalize the Greek version of the scale.
The LAD scale consists of 60 words separated into three columns of graded difficulty and increasing complexity, which the participants had to pronounce. The scale was administered by asking the person to read aloud and pronounce words consecutively from each of the three lists. Participants were given 5 seconds to read each word. When a participant needed more than 5 seconds to read a word, they were asked to proceed to the next word. Correctly pronounced words were counted as correct responses and given a score of 1; incorrectly pronounced words received a score of 0. The raw score was calculated by summing the scores from the three word lists, based on the number of correctly pronounced words. This total was then converted to a reading grade level using the conversion table provided in the instrument's score sheet [11].
The LAD score ranges from 1 to 60, based on the number of correctly pronounced words. Scoring is ordinal and not based on a Likert scale. The total score is then categorized into three levels according to the original LAD framework: 1–20 (low level), 21–40 (moderate level), and 41–60 (high level) [11].
In order to check the content validity, a pilot interview study was carried out with the participation of ten people with DM. Interviews were conducted by the primary researcher during routine visits to health centers. The observations and comments reported through interviews with participants were used to develop the subscales of the Greek version of LAD. In addition to pronunciation ability, two additional verbal subscales were introduced to assess knowledge and comprehension simultaneously. This decision was based on discrepancies observed during the pilot test between participants' pronunciation skills and their understanding of words and concepts. For example, a patient might be able to pronounce words like “ketones” or “glycogen,” but how can we determine whether they actually know or understand the meaning of these terms? For the additional subscales, the same scoring was applied.
Completing the Greek version of the LAD scale required 5 to 7 minutes, as there were no particular difficulties in understanding the instructions related to completing the demographic data and the scale.
Participants also completed a form with demographic and clinical characteristics, including gender, age, marital status, education, and employment. Comorbidities were recorded individually, allowing for multiple entries per participant.
2.4. Data Collection Process
Data collection was conducted through interviews. After obtaining informed consent, the researcher completed the questionnaires during participants’ routine visits to the health center. Participants were recruited upon their arrival. The scale was administered individually, with utmost respect, acknowledging that individuals with low or limited health literacy may be particularly sensitive to difficulties with reading and pronunciation. As such, they were treated with courtesy and sensitivity throughout the process.
2.5. Ethics Approval
The study was conducted after obtaining permission from the 2nd Health Region of Piraeus and Aegean, the Ministry of Health, Greece, and the responsible ethics and university research committee (Protocol No. 59947, October 30, 2019). Participants were informed both verbally and in writing about the principles of anonymity, confidentiality, voluntary participation, and the possibility of withdrawing from the study at any time, and they signed the consent form. In addition, the protection of participants’ data was ensured through the anonymous completion of questionnaires and the assignment of codes.
2.6. Statistical Analysis
The statistical package Statistical Package for Social Sciences (SPSS 22.0, IBM Corporation, Somers, NY, USA) was used for the statistical analysis of the data. To check the reliability of the questionnaire, the Cronbach's alpha coefficient was calculated. Descriptive and inductive statistical analysis was performed. Parametric tests, such as the t-test and ANOVA, were employed to analyze the data and determine statistical significance. These tests were chosen because they are appropriate for comparing group means and provide reliable p-values when the data meet assumptions of normality and homogeneity of variance. The level of statistical significance was set at p<0.05.
3. RESULTS
3.1. Demographics
A total of 58% of the participants were men with an average age of 67 years. The majority of participants were married (62%), retired or unemployed (84%), living with their families (68%), and 48% had graduated with primary education. Regarding the provision of counseling support, all participants reported some level of involvement from the attending physician, whereas nurse involvement was mentioned by 24% of respondents. Additionally, 24% of patients reported having no concomitant disease, while 20% reported cardiovascular conditions (Table 1).
3.2. The Validation of LAD
The Greek version of LAD was assessed in terms of its validity and reliability.
3.2.1. Descriptives of the Scale
The mean score for the “Pronunciation” subscale was 54.28 ± 4.34, for “Knowledge”, it was 56.76 ± 3.75, and for the “Comprehension” subscale, it was 48.92 ± 7.05 (Table 2). All participants achieved scores within the highest reading level category (41–60). Partial knowledge of the assessed words was evident in nearly all participants, as reflected by the high average score in the Knowledge subscale (56.76), approaching the maximum possible score of 60. In comparison, the Pronunciation subscale showed a slightly lower mean score (54.28), while the Comprehension subscale displayed a more noticeably reduced performance (48.92).
In terms of adaptive percentage performance in verbal assessment (Fig. 1), the “Knowledge” subscale was rated at 94.6%, “Pronunciation” at 90.5%, and “Comprehension” at 81.5%.
| Age (years) | Mean±SD | 67±23.10 | |
|---|---|---|---|
| - | - | N | % |
| Gender | Men | 29 | 58 |
| Women | 21 | 42 | |
| Marital Status | Married | 31 | 62 |
| Unwed/ widowed/divorced | 19 | 38 | |
| Accomodation | Alone | 16 | 32 |
| Family | 34 | 68 | |
| Εducation | Primary | 24 | 48 |
| Secondary | 17 | 34 | |
| Τertiary | 9 | 18 | |
| Εmployment | Εmployed | 8 | 16 |
| Unemployed/retired | 42 | 84 | |
| Counselling | Physician | 25 | 50 |
| Physician/internet/mass communication/social environment | 13 | 26 | |
| Physician/Nurse | 12 | 24 | |
| Comorbidities | None | 14 | 28 |
| Cardiovascular diseases | 10 | 20 | |
| Retinopathy | 9 | 18 | |
| Νeuropathy | 5 | 10 | |
| Cancer | 3 | 6 | |
| Αutoimmune disorder | 2 | 4 | |
| Other | 7 | 14 | |
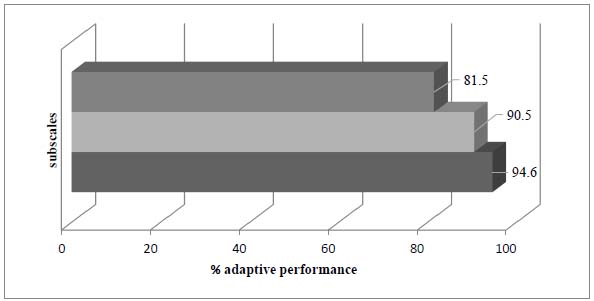
Percentage of adaptive performance in verbal assessment (knowledge: 94.6%; pronunciation: 90.5%; comprehension: 81.5%).
| LAD | Mean± SD* | Min | Max |
|---|---|---|---|
| Comprehension | 48.92±7.06 | 34 | 60 |
| Pronunciation | 54.28±4.34 | 42 | 60 |
| Knowledge | 56.76±3.75 | 38 | 60 |
| LAD | Age Group (years) | Mean±SD | P* |
|---|---|---|---|
| Knowledge | ≤67 | 55.67±2.73 | 0.047 |
| >67 | 57.77±4.31 | - | |
| Pronunciation | ≤67 | 52.17±3.89 | 0.001 |
| >67 | 56.23±3.85 | - | |
| Comprehension | ≤67 | 45.58±6.18 | 0.001 |
| >67 | 52.00±6.48 | - | |
| Knowledge | Employment | - | - |
| Εmployed | 59.50±1.07 | 0.023 | |
| Unemployed/retired | 56.24±3.86 | ||
| Pronunciation | Εmployed | 58.63±2.20 | 0.001 |
| Unemployed/retired | 53.45±4.16 | ||
| Comprehension | Εmployed | 56.38±5.88 | 0.001 |
| Unemployed/retired | 47.50±6.38 |
| - | Primary (N=24) |
Secondary (N=17) |
Tertiary (N=9) | - | - |
|---|---|---|---|---|---|
| - | Mean±SD | Mean±SD | Mean±SD | F* | P |
| Knowledge | 54.67±4.31 | 58.06±1.60 | 59.89±0.33 | 11.118 | <0.001 |
| Pronunciation | 51.17±3.82 | 56.06±2.11 | 59.22±1.20 | 28.473 | <0.001 |
| Comprehension | 43.58±5.14 | 51.41±3.43 | 58.44±2.24 | 45.122 | <0.001 |
3.2.2. Reliability
The reliability of the LAD scale was tested for the characteristics of stability and internal consistency.
3.3. Correlations between Demographics and LAD
No statistically significant differences were observed in relation to gender, type of accommodation and counseling, marital status, and comorbidities. In Tables 3 and 4, only the significant correlations are presented.
To assess differences in LAD subscale scores across age and employment status groups, independent-samples t-tests were performed (Table 3). Across all LAD subscales, participants younger than the median age of 67 had significantly higher scores compared to older individuals. Additionally, those who were employed scored significantly higher than those who were retired or unemployed. A significant difference (p < 0.001) was observed between employed individuals under the age of 67 and those who were older than 67, unemployed, or retired. Additionally, statistically significant differences were found between educational level and all LAD subscales (p < 0.001).
One-way ANOVA was used to examine differences in LAD subscale scores across education levels (primary, secondary, tertiary). Post-hoc comparisons were performed where appropriate. Post-hoc analysis revealed that in the “knowledge” subscale, primary education graduates scored significantly lower than both secondary (p = 0.004) and tertiary (p < 0.001) education graduates, while no significant difference was found between secondary and tertiary graduates. In the “pronunciation” subscale, significant differences were observed between all groups: primary and secondary (p < 0.001), primary and tertiary (p < 0.001), and secondary and tertiary graduates (p = 0.040). Similarly, in the “comprehension” subscale, significant differences were found between primary and secondary (p < 0.001), primary and tertiary (p < 0.001), and secondary and tertiary graduates (p = 0.001). In all cases, tertiary graduates had a higher score than secondary graduates, and those in turn scored higher than primary graduates (Table 4).
4. DISCUSSION
This study aimed to evaluate the validity and reliability of the Greek version of the LAD scale by applying it for the first time in a Greek population. The objective was to establish the scale as a practical tool for nurses and other healthcare professionals managing adults with diabetes mellitus (DM) in community settings. The Greek version demonstrated excellent internal consistency and test-retest reliability, suggesting strong potential for its future application in this population. However, the types of validity that could be assessed were limited, primarily due to the lack of a validated, comparable questionnaire in Greece and the consistently high scores observed across most items in the study.
Participants with DM demonstrated a notably high level of accuracy in pronouncing words and terminology related to DM commonly encountered in daily disease management. Despite the generally low educational level of the sample, most participants achieved high scores in both the knowledge and pronunciation components across all three word lists, which were organized in increasing order of difficulty. This performance may be attributed to the fact that the scale was translated into the participants’ native language, facilitating greater familiarity and comprehension.
This study represents an additional effort to translate and culturally adapt an HL assessment tool from English. In the context of DM care, accurate and quantitative assessment of HL is essential, as it directly supports effective self-management of the disease. A representative example of an HL assessment tool is the European Health Literacy Survey Questionnaire (HLS-EU-Q) [13], which has been translated into more than ten languages. However, many commonly used HL tools tend to assess only specific domains, primarily reading and writing skills, while often overlooking other critical competencies, such as verbal communication, navigating the healthcare system, and informed decision-making. Moreover, the approach to translation and cultural adaptation varies depending on linguistic, cultural, and methodological factors, as well as the nature of the tool being adapted [14].
The structure of health literacy assessment tools, their mode of administration, and the time required for completion are key factors that affect their applicability and effectiveness in both clinical and research settings [15]. Although the LAD scale is considered a valuable assessment tool, having been evaluated against instruments such as the Wide Range Achievement Test (WRAT) and the Rapid Estimate of Adult Literacy in Medicine (REALM), it has appeared in only a limited number of studies, and typically in combination with other assessment scales [2, 10, 16]. In contrast, other tools like the DNT-15 (Latino) have been more widely adapted, with the Spanish version developed specifically to address the assessment needs of Hispanic populations in the United States [17].
Translations of the LAD scale remain limited in the Western world, with the first known translation and cultural adaptation conducted in Arabic in 2020. In the Arabic version, minor modifications were made to a few words, which were rephrased or rearranged to improve clarity [12], though no subscales were added. The process of translating and adapting the scale into Arabic presented notable challenges due to significant cultural differences in language, customs, and dietary practices between the Western and Arab contexts. Consequently, specific terms had to be replaced to ensure both cultural relevance and semantic equivalence. Further revisions have been suggested to enhance cultural adaptation and maintain the intended conceptual meaning within the Arab cultural framework [12].
On the contrary, in the present study, the translation and rendering of the meaning of the words in Greek encountered no significant difficulties. The application of the LAD scale in the Arabic version took several minutes to complete, and no changes to the scale title or the included instructions were required. However, demographic data were obtained separately, as the LAD scale was administered concurrently with other scales. In the Arabic version of the LAD scale, the order of the words in the three lists was rearranged from their original sequence in the English version. However, such modifications were not necessary in the Greek adaptation, where the original word order was preserved.
The use of the LAD scale contributes significantly to the design and implementation of educational interventions in populations with DM to improve their self-care. In the research by Omar et al. (2020), an educational intervention was carried out in people with DM, through WhatsApp, in order to investigate the effect of the intervention on glycated hemoglobin (HbA1c) values. The LAD scale was also used in the research to assess the possible association of HL and numerical calculation ability related to DM and intervention results. The results showed no correlation between LAD scale scores and HbA1c values at baseline, three months, or six months post-intervention. However, the WhatsApp-based intervention proved effective for all participants, including those with low HL scores. This outcome may be attributed to the use of simple, easily understandable language and supportive visual aids, such as videos and images, designed to be accessible to all individuals with DM, regardless of their HL level [18].
The limitations of the study included its small sample, which limited the analyses, and the limited number of translations of the scale into languages. The scale was originally created in English [11] and was recently translated and culturally adapted in Arabic [12]. Additionally, there was a lack of sufficient international studies using the LAD, making it difficult to compare the analysis results.
The present study is unique in that it assesses the reliability and validity of a scale that has not been previously systematically used or tested. Additionally, the Greek version of the LAD includes two additional subscales, “knowledge” and “comprehension”, which are considered important for Greek adults with DM who are treated in the community. This Greek validation applies to adults with DM who speak the Greek language. Nevertheless, the scale requires further psychometric validation in other populations, settings, and countries. Validation of the LAD scale should be conducted with a larger and more diverse sample, ensuring greater gender and geographic representation, and ideally recruiting participants from multiple sites across Greece to enhance the generalizability and cultural applicability of the findings.
CONCLUSION
The Greek version of the LAD scale is an easy-to-use and reliable tool that can aid in assessing health literacy (HL) among Greek adults with diabetes mellitus (DM). By correctly utilizing the Greek LAD scale, nurses and healthcare professionals can help adults with diabetes better understand essential dietary and medical instructions related to their condition. This, in turn, enables the provision of person-centered care tailored to each individual’s level of health literacy and comprehension. In community and primary care settings, community nurses can employ the LAD scale to design and plan targeted educational interventions aimed at promoting more effective self-management of the disease. However, it is recommended that the scale’s validity parameters be reexamined in larger, more diverse samples and settings in future research.
AUTHORS’ CONTRIBUTIONS
The conceptualization of the study was carried out by M.M and A.K. Data curation was performed by M.M, A.K, and A.N. Formal analysis was conducted by E.V. The investigation was led by M.M. Resources were provided by M.M, A.K, and A.N. Supervision was overseen by A.K. Visualization was done by M.M, E.V, and I.T. The original draft of the manuscript was written by M.M, I.K, and I.T. Writing, review, and editing were performed by M.M, I.K, I.T, and A.K.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was performed after granted permission from the 2nd Health Region of Piraeus and Aegean, Ministry of Health, Greece, responsible ethics and university research committee (Prot No 59947/Oct 30th 2019).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

